
- Raised erythematous plaques covered with silvery scales
- Preferred locations: olecranon regions, knees, scalp, lumbosacral region
- Itching of varying intensity, sometimes very debilitating
- Depending on the natural pigmentation, the lesions may exhibit chromatic variations and generate residual post-inflammatory hyperpigmentation.
Psoriasis Guttata: Microlesions with Major Consequences
This variant, often observed in the pediatric population or young adults, is characterized by a rash resembling a multitude of droplets scattered mainly on the trunk, upper or lower limbs, frequently after an infectious episode such as streptococcal pharyngitis.
Distinctive features:
- Small papular lesions, resembling guttate lesions
- They are usually triggered by a prior bacterial infection (particularly with streptococcus).
- Less scaly than plaque psoriasis, but with a more widespread distribution
- Sometimes represents the initial manifestation of previously asymptomatic psoriasis.
Inverse Psoriasis: Discreet but Particularly Uncomfortable
In areas of skin flexure – axillary regions, inguinal folds, submammary region – a less conspicuous but extremely debilitating form develops: inverse psoriasis.
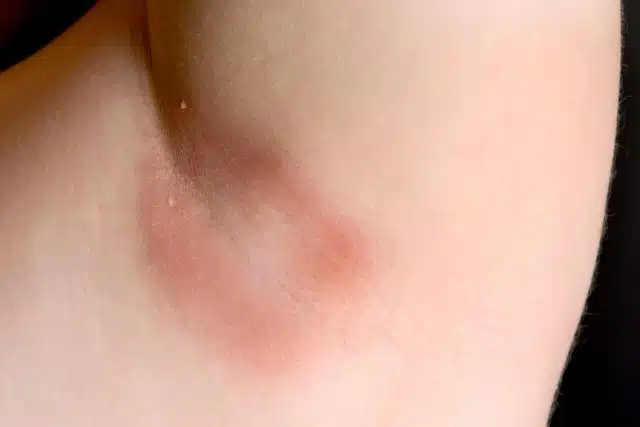
Clinical specifics:
- Erythematous plaques, with a smooth and shiny appearance
- Exacerbation by environmental heat, hyperhidrosis, and mechanical friction
- Increased predisposition to fungal superinfections
- The characteristic scales are absent, replaced by persistent irritation. The sensory experience is similar to that of continuous rubbing of damp textiles on a hypersensitive skin surface.
Pustular Psoriasis: Severe Skin Inflammation
Less common, this form presents a striking clinical picture: whitish vesicles containing pustular (non-infectious) material appear on a sensitized erythematous background. The distribution can be localized (palmar-plantar regions) or generalized.
Concerning clinical signs:
